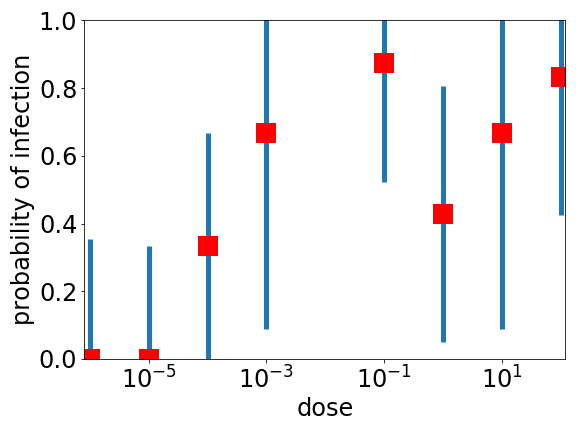
We don’t know the answer to the question in the title of this post, maybe only a few viruses are enough, maybe it is a hundred or a thousand. In fact, I am not sure we know the answer to this question for any infectious disease. I don’t think we know how many TB bacteria need to be inhaled to become infected, or how many noroviruses you need to pick up to become infected with the norovirus — also sometimes known as the winter vomiting bug. But for the norovirus at least we have a little data on how the probability you become infected increases as you increase the dose — see data by Teunis and coworkers plotted above. Note that the units of dose above are basically arbitrary so the absolute units are irrelevant but what is relevant is that the x axis is a log scale, and the doses vary by a factor of 100 million. Also note the very large (estimated) error bars* (in blue).
The error bars are large as this was a study of only 53 people, 22 of whom became infected, with 15 of these showing the symptoms of vomiting and diarrhoea. As noroviruses are I think not very dangerous to healthy adults, it was deemed ethical to deliberately infect people for the sake of science, but I guess for ethical and practical reasons they could only study 50, not the 10,000 you would need to get good statistics. Giving thousands of people diarrhoea was perhaps a step too far, which is fair enough.
So the statistics are terrible, but it is possible to see two things. The first is that the range of doses used is huge: they start seeing infection at a dose of 10–3 and the probability of being infected may or may not have plateaued at a dose of 102, a dose 100,000 times higher. The second is that they never see 100% infected, no matter how high the dose. It seems that some small-ish fraction of the population is essentially immune to at least this particular strain of the norovirus.
In the absence of much data it is hard to say whether or not the dose/infection probability curve for SARS-CoV-2 is similar or very different, to that of norovirus. It may well be that some people are much more resistant to SARS-CoV-2 than others, as they are to norovirus. As people vary quite a lot in terms of the genes for parts of their immune system, and what corona and noroviruses their immune system has seen before, person-to-person variability is to be expected. The infection probability even in superspreader events with SARS-CoV-2 never reaches 100 %, so it may well be that the variability is similar for corona and for noroviruses.
Person-to-person variability may also explain, at least in part, the very large range of doses. Perhaps because of this person-to-person variability, some people require much larger doses to become infected. In any case, the dose/probability of infection plot above is very far from what the Wells-Riley model I discussed in the previous post, predicts. Wells, Riley and coworkers assumed that there were ‘quanta’ of infectiousness, which are the same for everyone, and this may well be a very poor assumption.
* The points are from Teunis et al, error bars are my rough estimates.

2 Comments